Introduce yourself with your full name and title, confirm that you have the correct patient with their name and date of birth. Explain what you want you want to do and obtain informed consent
Request for chaperone
Ask for pain and if need painkillers
Ensure privacy and adequately expose the patient. If the patient is female, maintain her modesty
Check for walking aids around the bed and supports as such. Ask the patient to stand up and walk away from you and back.
Describe the gait of the patient.
From the front, with the patient standing in front of you, squat down to the level of the hips.
Observe for stance, shoulder and pelvis parallel to the floor.
What are the level of the shoulders: may indicate the presence of limb length discrepancy
Deformities
Muscle wasting
From the side
Is there any evidence of the deformity in the spine? Normal spinal curvatures and deformities in the spine like lordosis and kyphosis
Trochanteric area: examine for any swelling.
On the lateral aspect of the hip and limb: swellings, scars, sinuses, skin changes
From the back:
- Deformities in the spine : scoliosis
- Tell tale signs in the back: evidence of spinal deformities
- Levels of the posterior superior iliac spines/ iliac crests
- Sacral dimples- levels of the sacroiliac joints
- Level of the gluteal and thigh folds: indication to limb length discrepancy
- Any gluteal atrophy
-On posterior aspect of hip and limb- swelling, scars, sinuses
- Look for evidence of deformity if seen
Now since she is still standing we can straight away do the Trendelenburg instability test, or else wait til later to do it
Trendelenburg test: to demonstrate an ineffective abductor mechanism (gluteus medius weakness, dislocated or destroyed head of femir, nonunion of neck of femur, coxa vara).
Kneel in front of the patient and hold their pelvis. Ask the patient to alternatively stand on one leg. Normally the iliac crest on the side raised should rise. If it falls, it may be due to weakness of gluteal muscles
Ask the patient to lie down flat on the coach. From the front with the patient supine
- Attitude of the limb: position of various joints, direction and degree
flexed, abduted internally rotated--- posterior dislocation
externally rotated--- fracture neck of femur.
- Deformity of the hip if any and details therein
- Spine: evidence of exaggerated lumbar lordosis: level of shoulders
- ASIS: level of anterior superior iliac spines: abduction/ adduction deformities
- Femoral triangle examination: swelling and its description
- Presence of swelling scars and sinuses, dilated veins and description of each as on inspection of the hip and entire limb.
- On the side. see the trochanteric area. Confirm with the knee flexed.
- Trochanteric bursa- inflamed--- swelling/ fluid/ painful
- Muscle wasting
- Limb length discrepancy
- Galleazi's sign: flex knees to 90 degrees and hips and ankles at 45 degrees. Put malleoli at same level. Note level of knees. Parallel level of femurs and tibia.
- If the knees are at different levels, but tibia is parallel so discrepancy not above knee (ie its in tibia).
- If femurs are parallel, discrepancy not below knee ie in femur.
Palpation
Local rise of temperature over the area of interest. Check the normal side
Tenderness--- at the joint line--- by the side of the femoral pulse.
If it is very tender, do it gently. Do not make the patient cry
If cannot feel femoral pulsation- is it dislocation?
= flexion deformity
= internally rotated
= shortenimg
Tenderness over the greater trochanter- trochanteric bursitis
Confirm all inspectory findings in the spine and back- regarding spinal deformities, swelling, scars, sinuses, limb length discrepancy
Look for presence of lymph nodes whenever appropriate
Bony prominences: ASIS, greater trochanter (height, tenderness, width, surface of he greater trochanter in comparison to the opposite side), patellar height and medial malleolar level.
Bony irregularities: look for presence of bony irregularities and details of where such irregularities are palpated. Also look for any deformity of the bone and record direction of the deformity
Palpate for all peripheral pulses and look for motor and sensory disturbances in areas concerned
Vascular sign of Narath: in condition where the head or neck of the femur are not in place of are destroyed as a complication of a disease process, the femoral pulsation on the affected side is well felt.
When increased lumbar lordosis is present: indicates primary spinal deformity or an underlying fixed flexion deformity of the hip.
The degree of deformity has to be measured in degrees by doing the Thomas test. When ASIS is found to be at different levels, it indicates spinal deformity leading to pelvic obliquity or a fixed abduction or adduction deformity of the hip leading to obliquity of the pelvis. When ASIS on the affected side is at a lower level it indicates an abduction deformity on the hip and when at a higher level indicates an adduction deformity of the hip.
The degree of deformity has to be measured only after squaring the pelvis and unmasking the deformity. Deformity has to be quantified in degrees.
Movement
First do Active Movement, then only do passive movement.
You may put your left hand under the patient's spine to check if the patient is using the pelvis or spine during the movement phase.

Ask the patient to first do flexion which is normally up to 120 degrees. See if any pain.
Ask the patient to turn prone to check extension. Make sure you place the hand on the pelvis to fix it. Normal range is from 0-20 degrees.
Square the pelvis by placing your left hand over the patient's left hip.
Adduction: bring the foot to the opposite side, fully extended. 25 degrees from midline

Abduction: with the patient's leg fully extended, bring the leg closest to you 0-45 degrees from midline
Repeat for the opposite leg.

Internal rotation and external rotation. Repeat for other leg. Normal range is 25-45 degrees in and out.

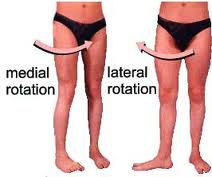
Flex the knee and hip to 90 degrees. Move the foot inwards for internal rotation and outwards for external rotation.
All the ranges of movements in all directions normally possible in the joint has to be measured in degrees.
Movements have to be recorded in a tabular column showing the movements on the right hand and the left sides in each direction and a column to record the difference foind in each directions.
This tabular column can also depict the power in each group of muscle eg flexors, extensors, abductors etc.
When fixed deformities are found
Movement in opposite direction is not possible.
Movements in the same direction as the deformity may be possible.
Eg when fixed abduction deformity is seen to be present, adduction at the hip will not be present and vice versa.
ALL MOVEMENT SHOULD BE RECORDED AS RANGE OF MOVEMENT WITH A DEFINITE START AND END POINT MENTIONED IN DEGREES.
Measurements
All bony prominences should be marked with a marking pen on both side before measurements
The tape should be placed gently on these points during measurements. Care should be taken to ensure that the points have not been moved under the examining fingers.
Apparent length: from the xiphisternum to the medial malleolus with the patient supine and lying down as straight as possible. In abduction or flexion deformity there may be apparent shortening.
True measurement of the entire limb in genuine shortening of the limb
1) Square the pelvis
2) Both limbs to be kept in similar positions when measuring
3) Measure from ASIS to the medial malleolus on each side
Segmental true measurement
1) Squared pelvis
2) Femoral length
- ASIS to the medial joint line
- The medial joint line is palpated with the knee in the 10-0 degrees of flexion when possible. The tibial tuberosity is identified and the examining fingers are un proximally on the tibia along the flare of the tibia
- A depression is felt as the fingers run proximally which is placed perpendicular to the axis of the femur on the medial and lateral aspects of the knees. This represents the medial and lateral joint line
This is confirmed by then moving the joint into flexion and extension whenever possible with the examining fingers still placed on the medial and lateral aspects of the knee. The movements are appreciated to be occurring at that level confirming it to be the joint line.
Tibial length
From medial joint line to the medial malleolus
Limb girth
If there is evidence of muscle wasting.
Bryant's triangle: to decide if there is supratrochanteric or infratrochanteric shorting. 1st draw a line joining the ASIS and the greater trochanter. Then one line is dropped perpendicularly to the bed from the ASIS. Join a line to that line. Compare with opposite side. If it is shorter, it signifies supratrochanteric shortening.
1st draw a line joining the ASIS and the greater trochanter. Then one line is dropped perpendicularly to the bed from the ASIS. Join a line to that line. Compare with opposite side. If it is shorter, it signifies supratrochanteric shortening.
1st draw a line joining the ASIS and the greater trochanter. Then one line is dropped perpendicularly to the bed from the ASIS. Join a line to that line. Compare with opposite side. If it is shorter, it signifies supratrochanteric shortening. Shoemaker's line:
Shoemaker's line:  Nelaton's line:
Nelaton's line: 
Special Test
Thomas test
DO NOT DO ON ANYONE WHO HAS HAD HIP REPLACEMENT
With the patient supine on a hard surface, look for evidence of excessive lumbar lordosis by looking for light passing through and through the lumbar area between the back and the couch
Pass the palm of the hand under the lumbar region. This cannot be done in a normal situation. If the palm can be passed under the lumbar area between the back and the couch it indicates excessive lumbar lordosis
With the palm under the lumbar back, flex the hip on the unaffected side through its full range of flexion and continue to flex it beyond till the lumbar back just touches the hand. Notice the hip on the affected side flexing with this manoeuvre.
With the unaffected hip in position of flexion, passively extend the hip on the affected side as much as possible without allowing the patient to arch the back. The angle that the back of the thigh makes to the couch on the affected side is the amount of fixed flexion deformity of the hip.
Incomplete extension quantify fixed flexion deformity in the hip.
SUMMARISE
Inspect for
walking aids
attitude
SSSW
deformity
shoulder tilt or lumbar lordosis
trendelenburg test
gait
Palpate for
temperature
tenderness
ASIS
Iliac crest
PSIS
Sacroiliac joint
Sacroiliac joint
greater trochanter
Greater trochanter
Adductor area
Bryant's triangle
Shoemaker
Nelaton
Measurement
Apparent length
Square pelvis for true length
Muscle wasting
Movement
Flexion 0-140
Extension 0-20
Internal rotation 0-30
External rotation 0-40
Abduction 0-45
Adduction 020
Extension 0-15
Special test:
Thomas test
Random Notes
Hip is innervated by L2-S1
L2 also innervates the knee, hence hip pathology may have referred pain in the knee
Spine gives off L3
How to locate the hip- femoral triangle
Squaring of pelvis--- why is it called squaring?
iliac crest is on the same level.Limbs in same position.
Abduction- shortens the limb
Adduction- lengthens the limb.
What are causes of true shortening of limb?
= fractures
= hip arthroplasty
= slipped upper femoral epiphysis
= hip dislocation
= juvenile osteoarthritis
= septic arthritis
= loss or articular cartilges
= congenital coxa vara
= growth disturbances.
Patient cannot abduct and internally rotate. What do you suppose it is?
Osteochondritis of femoral head- Perthes disease.
What are causes of true shortening of limb?
= fractures
= hip arthroplasty
= slipped upper femoral epiphysis
= hip dislocation
= juvenile osteoarthritis
= septic arthritis
= loss or articular cartilges
= congenital coxa vara
= growth disturbances.
Patient cannot abduct and internally rotate. What do you suppose it is?
Osteochondritis of femoral head- Perthes disease.
No comments:
Post a Comment