Non specific organisms (pyogenic)
- strep
- staph
Specific organisms
- TB
- Syphilis
- Salmonella
- fungal osteomyelitis, actino and madura mycosis
- parasitic hydatid cyst
Spread of infection
- Haematogenous
- from a distant site in the body throat infection
- Direct
- Atmospheric air-open fracture
- Neighbouring focus
Mastoiditis from middle ear infection
Dental root infection producing osteomyelitis of the mandible
- Iatrogenic
Following surgery on the bone for some other reason- ORIF
Osteomyelitis is comparatively more common in children/ infants.
If it does occur in an adult, the commonest site is the thoracolumbar spine
Other bones can be affected in diabetes mellitus, malnutrition, drug addiction, leukaemia and other immunocompromised situations
Clinical types of OM
Acute pyogenic OM
Chronic OM
Primary subacute OM
Acute flare up of chronic OM
Pyogenic OM
- Problem of childhood and adolescents
- undernourished children and debilitated adults
- common organisms- staph aureus and strep pyogenes
- In children <4 yrs old, haemophilus influenzae
- unusual organisms seen in drug addicts---
- in sickle cell anaemia, they have a predilection for salmonella OM
- Haematogenous spread is common.
- Focus is usually from infectiosn like impetigo, septic tooth, throat infection, infected umbilical cord
 Pathogenesis
Pathogenesis
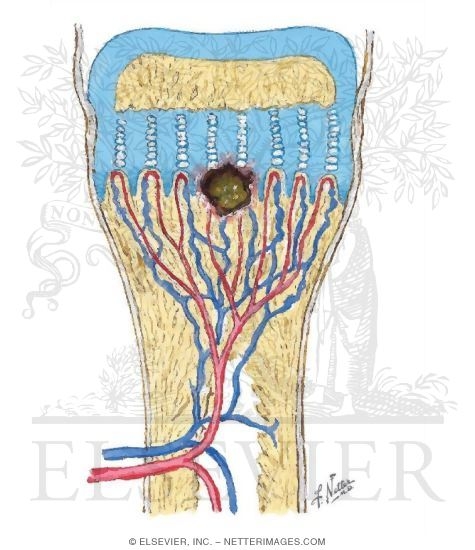
Infection commonly starts in the metaphysis of a bone
This is due to the peculiar anatomy at this zone
- arteries tend to loop causing
- vascular stasis, which
- favours colonisation
Furthermore, there is less phagocytosis in the metaphysis
Organisms colonises in the bone
Causes inflammation
Phagocytic reaction, exudation of fluid, vascular congestion
Intraosseous pressure increases
Pain, obstruction to blood flow, vascular thrombosis
Pus forms in the bone and is forced out through the Volkmann;s canal with increased intraosseous pressure to the subperiosteal space
Subperiosteal abscess
 The subperiosteal abscess bursts through the periosteum into the soft tissue, forming a sinus
The subperiosteal abscess bursts through the periosteum into the soft tissue, forming a sinus
It may also burst into a joint causing septic arthritis
Strips the periosteum--- periosteal blood supply is lost--- sequestrum
Intramedullary extension of the pus
Intraosseous blood supply cut off
Dead bone- Sequestrum
Small dead bone absorbed by granulation tissue and osteoclastic activity
Large gradually separated from living bone destroyed and extruded
In certain situations like hip joint the metaphysis is intracapsular and infection can easily seep into the joint
In infants and adults, vascularity pattern--- intracapsular infected epi and metaphysis---- spread to the joint
Penetrates the periosteum---- track along soft tissue and penetrates the capsule
common vascularity between epiphysis/ metaphysis and synovium
Disruption of cartilage and spread
Pathological fracture
Healing takes place at any stage
- antibiotics
- natural persistence
Healing in early stage--- exudate is reabsorbed and new bony trabeculae formed
Organism, of lesser virulence or host demonstrates increased resistance--- result in formation of persistant abscess surrounded by fibrous membrane and walled by ring of dense bone called Brodie abscess.
When sequestrum has formed exudation continues til it is absorbed or extruded
Wall off area of infection may flare up again later---- chronic OM
Clinical features
antecedent infection
irritable, restless, vomiting, high grade fever with chills
pseudoparalysis of the limb
at first, no swelling later+ infdicates subperiosteal abscess formation
affected metaphysis is tender
Fluctuation present after abscess comes to soft tissue effusion in adjacent joint- sympathetic effusion
If infection continues unabated- septicaemia- fatal termination.
Laboratory findings
- Haemoglobin: low
- Total WBC: as high as 30 000 with leucocytosis
- ESR: high
- Blood culture: demonstrates presence of bacteraemia
Radiology of APOM
- initally, up to 10 days- normal
Later: localised areas of destruction in the metaphysis extending ti the diaphysis- moth- eaten appearance
Periosteal elevation: multiple laminations of bone deposition parallel to the bone- appears like the onion peel appearance- seen in Ewing;s sarcoma .
Late sign: osteoporosis with a localised segment of apparently increase density eg femoral head.
Other Investigations
MRI
CT Radiography
Diagnosis and needle aided drainage of pus for culture and sensitivity from inaccessible parts- vertebra
Radionuclide examination
Technetium phosphate- Tc99m
Positive within hours to days
initially cold spot later hot spot
depends on vascularity to the part and in the presence of increased IOP may not reach the affected part.
Gallium 67
Taken up by leucocytes
independent of vascular tree
also taken up by inflamed soft tissue and hence difficult to differentiate between cellulitis and osteomyelitis
Indium 11 labelled leucocytes
taken up by leucocytes
most suitable more sensitive
requires technical expertise and is time consuming.
MRI
Useful in early detection of osteomyelitis and soft tissue extension
DDX
Rheumatic fever: onset more gradual, consitutional symptoms less, acute and confined to the joint, polyarticular, response to salicylates and ACTH is dramatic. Antibiotics have no effect.
Ewings sarcoma: fever, leucocytosis, subperiosteal reaction- onion peel appearance, destruction confined to the diaphysis, responds to radiotherapy, biopsy shows tumour cells.
Acute septic arthritis: fluid accumulation in the joint occurs earlier, pain and inflammation limited to the joint, joint movements grossly restricted, aspiration reveals purulent synovial fluid
Treatment: Early diagnosis with a high degree of suspicion is beneficial and necessary
Blood for investigations are collected and high doses of antibiotics are started as early as possible.
Antibiotics are changed later if necessary as per culture and sensitivity reports
Immediate drainage is of paramount importance and is done before signs of subperiosteal infection is seen.
To wait is to invite trouble and disaster. Maximum waiting period allowed is 24 hours SOS to improve general condition patient.
Immediate drainage by opening a cortical window at the suspected site.
Closed continuous drainage for 24-48 hours.
Or leave the wound open and allow secondary healing
Prolonged antibiotics as per culture and sensitivity report for minimum period of 6 weeks with initial 2 weeks of parenteral antibiotics.
COMPLICATIONS
Acute osteomyelitis invariably ends up as chronic osteomyelitis
Septicaemia and fatal end
Multifocal osteomyelitis in debilitated individuals- rare
After an attack of acute osteomyelitis recurrence of infection is a rule- the interval may vary.
Once an osteomyelitis always an osteomyelitis
Acute OM leading to chronic OM
Haematogenous infection with a low virulence organism may be chronic from the beginning
Infection from an external wound usually causes chronic osteomyelitis
Pathology
Repair when incomplete persistance of infection
Repair process- hyperaemia formation of granulation tissue and aborption of necrotic cancellous ad cortical bone.
When sequestrum is small and infection is controlled sequestrum gets resorbed
When large and infection persists- it separates out and lies in a cavity
The surrounding tissue attempts to wall off infection--- forms thick bony wall--- called the involucrum
Pathology
Involucrum has multiple openings called cloacae, openings for exudate, debris and sequestra to drain though the sinus.
Once sequestrum is extruded- infection is better controlled and settles down.
TYPES OF SEQUESTRUM
STIR BCD
Sandy ------ tuberculur OM of the vertebra
Tubular ------ tubercular OM of the long bone
Ivory --------- syphilitic osteomyelitis
Ring ---------- stump/ skeletal traction
Black --------- prolonged exposure of bone
Cortical ------ pyogenic OM adults
Diaphyseal --- pyogenic OM- children
Clinical features
In the period of inactivity no symptoms
Fever, pain, swelling and tenderness of bone
Sinuses discharging pus and bony spicules- sequestrum
Bone is thick, irregular or may be deformed
Skin dusky thin and scarred.
Muscles are scarred and contracted- produce deformities of adjoining joints
Radiology
Moth eaten appearance
Osteoporotic bone
Sequestrum
Involucrum
Bone thick and irregular
Bone may be deformed
Pathological fracture
Other Investigations
Sinogram
Traces the sinus tract and helps planning of surgery and removal of entire tract to prevent recurrence.
Sequestrectomy and saucerisation
Scondary healing of wound
Prolonged antibiotic- minimum of 6 weeks to 3 months according to culture and sensitivity report with initial parental antibiotics.
COMPLICATIONS
Acute flare up chronic osteomyelitis
Squamous cell carcnima of chronic discharging sinus
Contracture of muscle producing deformity of joints
Stimulation/ destruction of growth plate leading to discrepancy of limb length or deformities
Pathologic Fracture
Septic arthritis of adjacent joint- deformity and ankylosis
Amyloidosis
Brodie's abscess
Described by brodie in the tibial metaphysis in 1832
Indicates subacute pyogenic osteomyelitis usually of staphylococcal origin
Commonly seen in children- boys
Commonly affects the ends of the tibial bone
ABscess varies from 1cm-4cm in diameter
Radiologically seen as cavity surrounded by dense ring of bone.
Appropriate antibiotics may decrease the size of the lesion
If pain persists- may require surgical decompression of the abscess.
Great post, I appreciate you and I would like to read your next post. Thanks for sharing this useful information
ReplyDeleteback posture corrector
Vitamin A is one of the useful resource which used different kinds of disease herbal remedies it also play a very important role in the Herbal Treatment for Osteomyelitis .
ReplyDeleteHerbal Treatment for Osteomyelitis information about the Symptoms, Causes and Diagnosis. Natural Herbal Treatment for Osteomyelitis with Herbal Product Osteton Natural Supplement for infection of the bone. Treatment of this problem controls the Causes of Osteomyelitis.
ReplyDelete