Spinal nerves attach to the spinal cord via roots.
The dorsal root has only sensory neurons, attached to the cord via rootlets and it has a dorsal root ganglion
The ventral root has only motor neurons, no ganglion. All cell bodies of motor neurons found in the grey matter of the spinal cord.
Spinal nerves contain thousands of nerve fibres which are all mixed nerves having both sensory and motor neurons. They connect to the cord and supply muscles and structures of the body
.
Rami are lateral branches of a spinal nerve. They contain both sensory and motor neurons. There are two major groups: the dorsal ramus through which neurons innervate the dorsal regions of the body; and the larger ventral ramus which innervates ventral regions of the body. They braid together to form plexuses. A nerve plexus is nothing more than a system or network of connected nerve ibres that link spineal nerves withs pecific areas of the body. It is a network of ventral rami.
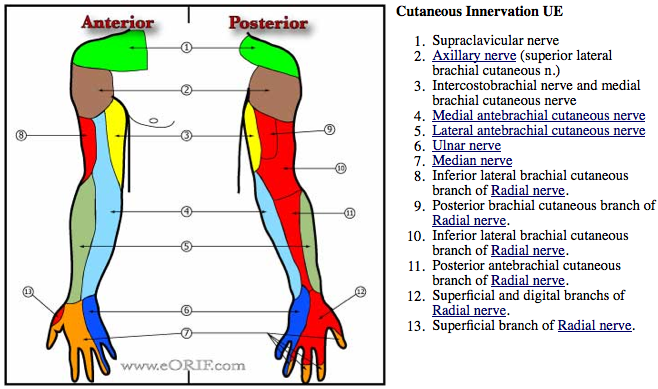
The brachial plexus is formed by the ventral rami of the spinal nerves C5-T1.These form 3 trunks that separate into 6 divisions then form cords that give rise to nerves. It is a 15cm long spinal column to the axilla and is responsible for cutaneous and muscular innervation of the entire upper limb and pectoral girdle. It proceeds through the neck, the axilla and into the arm.
Major nerves arising from them is Axillary, Radial, Musculocutaneous, Ulnar and Median
Root value of lateral cord and all its branches is C5,6, 7
Root value of medial cord and all its branches is C8 T1, except Ulnar nerve has some contribution from C7 too
Root value of posterior cord and its branches is C5, 6, with 2 exceptions:
Thoracodorsal nerve- C6,7, 8
Radial nerve- C5,6,7,8,T1
Root value of upper trunk and its branches is C5,6
BRANCHES
Lateral cord: LML
Lateral pectoral nerve
Musculocutaneous nerve
Lateral root of median nerve
Medial Cord
M4U
Medial pectoral
Medial cutaneous nerve of arm
Medial cutaneous nerve of forearm
Medial root of median nerve
Ulnar nerve.
Posterior Cord
ULTRA
Upper subscapular
Lower subscapular
Thoracodorsal
Radial nerve
Axillary nerve.


.png)
TESTING EACH MUSCLE SEPARATELY
Trapezius (middle):
O: spinous process of T1-5
I: medial margin of acromion and superior lip of spine of scapula
A: Scapular adduction and stabilisation
N: Spinal portion of cranial nerve XI
T: Patient prone
Trapezius (lower): CN XI- Spinal accessory nerve--- Shrug
O: spinous processes of T6-12
I: tubercle at apex of spine of scapula
A: rotation upward of the scapula
N: spinal portial of cranial nerve XI (accessory) ventral ramus C2-4
T: Pt prone with shoulder at edge of table, fix one hand below the scapua on the opposite side
Supporting the weight of the arm, the examiner places the scapula in a position of adducting with some lateral position. When support is released if the scapula remains adducted placed pressure in direction of abducted.
Serratus anterior:O: Outer surfaces & superior borders of ribs 1–8/9
I: Costal surface of medial border of scapula
A: Scapular abduction, upward rotation while also holding medial border against ribcage
N: Long thoracic, C5–8
T: Patient supine
No Fixation needed, unless shoulder or elbow musculature is weak; in this case arm would be supported in the perpendicular position
Test: Abduction of the scapula projecting the upper extremity anteriorly. Pressure
Against the subjects fist or elbow downward through the extremity in the direction of scapular adduction, slight pressure can ne added to the lateral border of the scapula
Rhomboideus major and minor
Middle Deltoid
- O: Anterior border, superior surface & lateral one third of the clavicle
- I:Deltoid tuberosity of humerus
- A:Abduction of the glenohumeral joint
- N: Axillary, C5–6
- T: Glenohumeral abduction without rotation
- Pressure: Against the dorsal surface of the distal end of the humerus if the elbow is flexed, or against the forearm if the elbow is extended
Anterior Deltoid
- O: Lateral margin & superior surface of acromion
- I: Deltoid tuberosity of humerus
- A: Flexion of the glenohumeral joint & medially rotate when supine
- N: Axillary, C5–6
- T: Patient Supine
- If the scapula is not propertly stabilized by the serratus anterior & the trapezius then the examiner should stabilize the scapula
- Glenohumeral abduction in slight flexion & medial rotation; one hand of the examiner is placed under the patient's wrist to make sure that the elbow is not lifted by reverse action of the wrist extensors which may occur if the patient is allowed to press the hand down on the chest
- Pressure Against the anterior surface of the arm just above the elbow in the direction of adduction toward the side of the body
Posterior Deltoid
- Origin
- Inferior lip of posterior border of the spine of the scapula
- Insertion
- Deltoid tuberosity of humerus
- Action
- Extend the glenohumeral joint & in a prone position cause lateral rotation
- Nerve
- Axillary, C5–6
- Patient
- Prone
- Fixation
- The scapulamust be held stable by scapular muscles or by the examiner
- Test
- Horizontal abduction of the shoulder with slight lateral rotation
- Pressure
- Against the posterolateral surface of the arm in a direction obliquily downward midway between adduction & horizontal adduction
Supraspinatus Origin
O short head - apex of coracoid process of scapula, long head- supraglenoid tubercle of scapula
I Tuberosity of radius and aponeurosis of biceps brachii
A Flexes the shoulder joint and the long head may assist with abduction if the humerus is laterally rotation
N Musculocutaneous C5-6
T Patient supine or sitting. Examiner places one hand under elbow to cushion it from table pressure. ELbow flexion slightly less than or at right angle with forearm in supination
Brachialis
O: Distal half of anterior surface of humerus and medial and lateral intermuscular septa
I: Tuberosity and coronoid process of ulna
A: With the origin fixed, flexes the elbow joint moving the arm towards the humerus. With the insertion fixed, flexes the elbow joint moving the humerus towards the forearm
N: Musculocutaneous, and a small branch from radial C5-6
T:
Coracobrachialis
O: apex of coracoid process of scapula
I: Medial surface of middle shaft of humerus, opposite deltoid tuberosity
A: Flexes and adducts the shoulder joint
N: Musculocutaneous C6-7
T: Shoulder flexion in lateral rotation with the elbow completely flexed and foream supinated
Pressure: against anteromedial surface of the lower third of the humerus in the direction of extension and slight abduction
Triceps
O: long head- infraglenoid tubercle of scapula... lateral head- lateral and posterior surface of proximal half of humerus and lateral intermuscular septum..... medial head- distal two thirds of medial and posterior surface of humerus below the radial groove and from medial intermuscular septum
I: Posterior surface of olecranon process of ulna and antebrachial fossa
A: Extends the elbow joint, with the long head assisting in adduction and extension of the shoulder joint
N: Radial, C6,8,T1
T: Patient supine or prone. Shoulder abducted to 90 neutral with regard to rotation and supported between the shoulder and elbow by the table. Extension of the elbow joint to just short of full extension
Pressure against the forearm in the direction of flexion/

MEDIAN NERVE
High Median Nerve Palsy: Injury proximal to the elbow: This will cause paralysis of all the muscle supplied by the median nerve in the forearm and hand as well as sensory deficit in the skin of the hand
Low median nerve palsy: (injury in the distal third of the forearm) – sparing of forearm muscles, but the muscles of hand will be paralysed, anaesthesia over the median nerve distribution in the hand
It supplies no muscle in the arm and non in distal 1/3 of forearm.
In proximal 1/3: All the flexor muscles of the forearm except he flexor carpi ulnaris and medial half of flexor digitorum profundus.
In hand: Three thenar muscles and the first 2 lumbricals.


Deformity, swellings, muscle wasting, scas esp carpal tunnel release scars, skin changes.
Ask patient to make a fist. Patient unable to flex the thumb, index and middle finger
 |
| POINTING INDEX due to paralysis of FDS and lateral half of FDP of index finger which occurs in median nerve palsy at a level proximal to the elbow. The other fingers can be flexed due to functional ulnar nerve. |
 |
| Ape hand deformity |
| anterior interosseouus nerve palsy following the use of elbow crutches |
Special Tests:
Screening test: Kumar's sign--- Radial nerve for wrist extension, ulnar nerve for finger abduction and median nerve for opposition
1. Flexor pollicis longus: Ask patient to flex the terminal phalanx of the thumb against resistance while the proximal phalanx is kept steady by the examiner
 |
| Flexor pollicis brevis |
2. Flexor digitorum superficialis and lateral half of flexor digitorum profondus
Ask the patient to clasp his hand, the index finger will remain straight, ‘pointing index’. Both the finer flexors are paralysed, medial half of the flexor digitorum profundus (ulnar nerve) makes flexion the other fingers possible
| flexor digiti minimi |
3. Flexor carpi radialis
Palmar flexion at the wrist occurs in the long axis of forearm. Paralysed flexor carpi radialis, the wrist deviates to the ulnar side while palmar flexion occurs. One cannot feel the tendon of flexor carpi radialis getting taut

4. Abductor pollicis brevis
| testing abductor pollicis brevis |
Patient is ask to lay his hand flat on the table with palm facing the ceiling. A pen is held above the thumb and the patient if asked to touch the pen with tip of this thumb. ‘pen test’
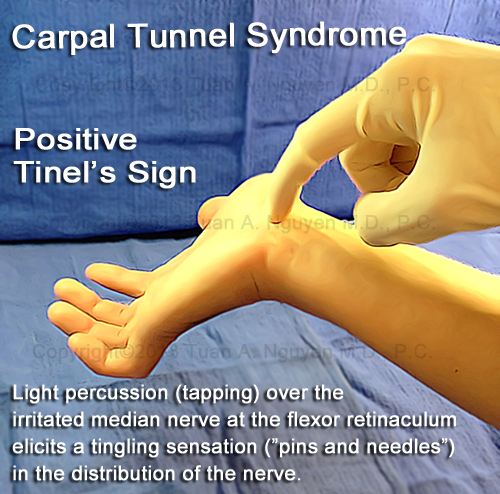
Tests for carpal tunnel syndrome
1. Phalen's test and Reverse Phalen's test:
The patient is asked to hold their wrist in complete and forced flexion (pushing the dorsal surfaces of both hands together for 30-60 seconds. The lumbricals attach in part to the flexor digitorum profundus tendons. As the wrist flexes, the FDS contracts in a proximal direction, drawing the lumbricals along with it. In some individuals, the lumbricals can be dragged into the carpal tunnel with flexor digitorum profundus contractions. As such Phalen's manoeuvre can moderatlry increase the pressure in the carpal tunnel via this mass effect, pinching the median nerve between the proximal edge of the transverse carpal ligament and the anterior border of the distal end of the radius.
By compressing the median nerve within the carpal tunnel, characteristic symptoms (such as burning, tingling or numb sensation over the thumb, index, middle and ring fingers) conveys a positive test result and suggests carpal tunnel with this manoeuvre, this test cannot be perfectly sensitive or specific for carpal tunnel syndrome.

Reverse Phalen's test
Patient maintain full wrist and finger extension for two minutes. The reverse Phalen's test significantly increases pressure in the carpal tunnel within 10 seconds of the the change in wrist posture and the carpal tubbel pressure has the tendency to increas throughout the test's duration. In contast, the change in carpal tunnel pressure noted in the standard Phalen's test is modest and plateaus after 20-30 seconds.
The average pressure change for Phalen' stest at one and two minutes was only 4 mmHg. The average pressure changes in the carpal tunnel for the reverse Phalen's test were 34mmHg at one minute into the test and 42mmHg at the 2 minute point.
The extended wrist posture significantly changes the pressure within the carpal tunnel and may be more useful as a provocative examination manoeuvre. Reverse Phalen;s manoeuvre results in a significantly higher intracarpal canal hydrostatic pressure as compared to a traditional Phalen's. THis is thought to add sensitivity to conventional screening methods.

2. Tinel's sign

5. Carpal tunnel compression test
With the patient's arm in supination, the examiner applies pressure with his/her thumbs over the median nerve within the carpal tunnel. This is located just distal to the wrist crease. A positive test occurs when the patient complains numbness and tingling in the median nerve distribution within 30 seconds. The examiner records the time of onset for the symptoms.
With patient's arm in supination
| Durkan's compression test |
ULNAR NERVE
 |
| ulnar claw hand (Main en griffe) |
THE CLOSER TO THE PAW THE WORSE IS THE CLAW
 |
| Wasting of hypothenar muscle |
SITE OF LESION
Forearm: High nerve lesion
 Muscular:
Muscular:Flexor carpi ulnaris:
Tendon don’t stand out
Flex wrist against gravity: RADIAL DEVIATION of wrist
Flex wrist against resistance: Tendon CANNOT be felt
Cutaneous branches
Palmar branch
Dorsal branch
*Test the exclusive areas
HANDS
Divides as it passes above flexor retinaculum
2 main branches:
- superficial terminal branch
Muscular branch: palmar brevis difficult to asses, no specific test
Cutaneous branch: two palmar digital nerves
- deep terminal branch
Deep terminal branch: MUSCULAR branch
Hypothenar muscles:
Abductor digiti minimi:
Keep hands FLAT and PALM up on

2. Flexor digiti minimi:
Position – hand in supination.
Stabilize – the hand.
Resist – small finger metacarpal-phalangeal flexion by applying force over palmar proximal phalanx (in the

3. Opponens digiti minimi:
Position – the hand palm up.
Stabilize – the hand and first metacarpal.
Resist – against opposition of the
/ODM---IMG_0546.jpg)

Interossei
1. Egawa Test: This is for dorsal interossei (abductors) of the middle finger. With the hand kept fla on a table palma surface down, the patient is asked to move his middle finger sideways.
2. Card Test: THis is for palmar interossei (adductors) of the fingers. In this test, the examiner inserts a card between two extended fingers and the patient is asked to hold it as tightly as possible while the examiner tries to pull the card out. The power of adductors can this be judged. In case of weak palmar interossei, it is easy to pull out the card. First dorsal interosseus muscle can be separately examinated by asking the patient to abduct the index finger against resistance.
3. Test for 1st dorsal interosseous
 Ask the patient to abduct the index finger against resistance.
Ask the patient to abduct the index finger against resistance.4. Froment's sign

The patient is asked to grasp a book between the thimb and index finger. Normally a person will grasp the book firmly with thumb extended, taking full advantage of the adductor pollicis and the first dorsal interosseous muscles. If the ulnar nerve is injured the adductor pollicis will be paralysed and the patient will hold the book by using the flexor pollicis longus (supplied by median nerve), in place of the adductor. This produces flexion at the interphalangeal joint of the thumb. This becomes more pronounced if the examiner tries to pull the book out while the patient tries to hold it. This sign is known as Froment's sign or the book test.
Amazing article :)
ReplyDeleteits really good thing you have shared thanks for info
BRACHIAL PLEXUS