
The fun thing about fractures of the shaft of the humerus, is that the humerus is a typical long bone. When studying fracture classification, all types can occur with this one. Hence in this topic I will refresh some basics.
1. What is a fracture?
A fracture is a complete or incomplete break in the structural continuity of a bone.
2. Classify fractures
Depending on its relationship with the external environment
A. Open: AKA a compound fracture: A fracture with a break in the overlying skin and soft tissues, leading to the fracture communicating with the external environment. It can be open internally or externally.
- Internally open (from within): the sharp fracture end pierces the skin from within resulting in an open fracture
- Externally open (from outside): the object causing the fracture lacerates the skin and soft tissues over the bone, as it breaks the bone, resulting in an open fracture.
B. Closed: AKA a simple fracture. A fracture which does not communicate with the external environment. Skin and soft tissue intact
A. Complete
B. Incomplete
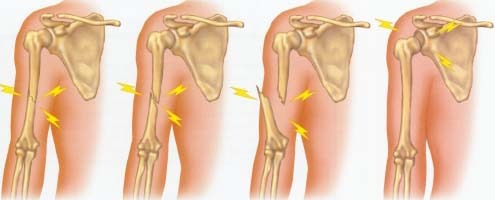
 Depending on the line of the fracture:
Depending on the line of the fracture:- Transverse- perpendicular force to long axis of the bone
- Oblique- bending force which has in addition a component along the long axis of the bone
- Spiral- fracture line runs spirally in more than one plae. Such a fracture is caused by a primarily twisting force.
- Comminuted- multiple fragments. Caused by a crushing or compression force along the long axis of the bone.
- Segmental: two fractures in one bone but at different levels.
- Compression
- Avulsion
- Impaction
Depending on displacement
- Undisplaced:
- Displaced
Depending on complexity of treatment
Simple: a fracture in two pieces, usually easy to treat is called simple fracture eg a transverse fracture of humerus
Complex: a fracture in multiple pieces usually difficult to treat, is called complex fracture eg a comminuted fracture of tibia.
FRACTURE SHAFT OF HUMERUS
This is a common fracture in patients at any age.
How it happens: It usually sustained from an indirect twisting or bending force- as may be sustained in a fall on outstretched hand or by a direct injury to the arm.
A fall on outstretched hand with a twist causes spiral fracture.
A fall on the elbow with the arm abducted exerts a bending force, resulting in an oblique or transverse fracture.
A direct blow can cause either a transverse or a comminuted fracture.
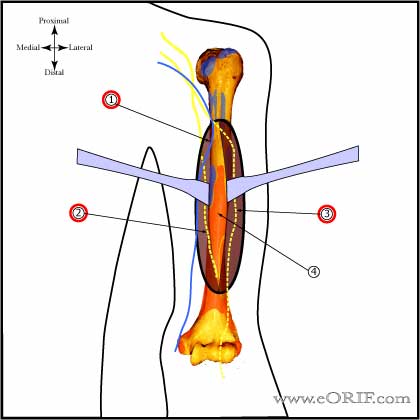
Anatomy: The humerus is a typical long bone. The upper half of the shaft is roughly cylindrical and begins to flatten in its lower half in the anterior posterior direction. The deltoid muscle is inserted on the deltoid tuberosity on the anterolateral surface of the bone, just proximal to its middle third. The posterior surface is crossed obliquely by a shallow groove for the radial nerve.
The humerus is surrounded by muscles. This has the following clinical relevance
i) the incidence of compound fractures is low
ii) the union of the fractures occurs early because a bone so well surrounded by muscles has a rich periosteal blood supply.
iii) some degree of malunion is masked by the thick muscle cover.
Displacements
Lateral angulation is common because of the the abduction of the proximal segment by deltoid muscle. This angulation is further increased by the tendency of the patient to keep the limb by the side of his chest resulting in adduction of the distal segment. Often, distraction occurs at the fracture site because of the gravity.
How patient presents:
Arm painful and swollen
Deformity
Loss of function
Signs: tenderness, abnormal mobility, crepitus,
signs of radial nerve injury
INVESTIGATIONS
XRay humerus AP and lateral view
 |
| Segmented fracture |
 |
| Comminuted spiral fracture |
| Oblique fracture of shaft of left humerus |
 |
| Spiral fracture of shaft of left humerus |
| Transverse fracture of shaft of left humerus |
How would you manage it?
Conservative: 70-80% of fractures can be managed non operatively, with an expected rate of union of 90-100%
Indication: closed fracture with no radial nerve palsy.
If it is a closed fracture with radial nerve palsy, do a closed reduction, put a U cast and a cock up splint, and explore after 8 weeks if no recovery ensues.
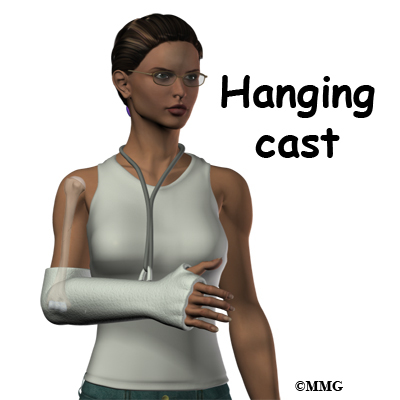
Reduction and POP cast: U cast "hanging am" cast.
If the fracture is below the deltoid insertion: proximal fragments are adducted. U cast or hanging arm cast
If the fracture is above the deltoid insertion: the proximal fragments are adducted by pectoralis major and latissimus dorsi: U cast
Acceptable alignment: Angular deformity of 2 degrees in lower and middle third and 30 degrees in upper third is acceptable.
AP angulation- 20 degrees
Varus- 30 degrees
Shortening- 3cm
Little functional deficit.
 |
| Hanging U slab |
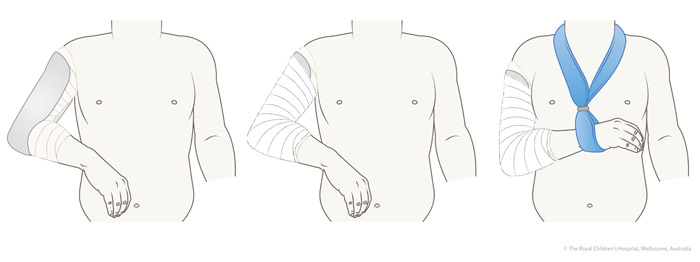 |
| Hanging U slab plaster of paris |
 |
| Hanging arm cast with cuff and collar |

Operative
Indication
- polytrauma
- multiple fractures
- floating elbow
-open fracture and radial nerve injuries
Method
CLosed reduction and internal fixation
Open reduction and internal fixation with plates and screws
Intramedullary nailing is another method of internal fixation
External fixation: open, contaminated fractures implants used
DC plate, rush nail, interlocking nail
preferably inserted for below, just above olecranon fossa
If insertion far above the greater tuberosity, it may impair shoulder movement.

COMPLICATIONS
Early/ Immediate
Vascular injury
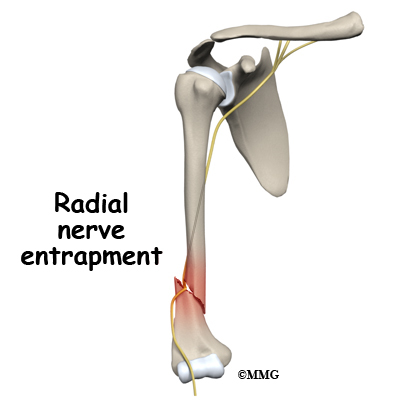
Nerve injury: radial nerve palsy 11%. Occurs especially in spiral fracture of the distal third of the humerus.
Late
Non union: inadequate immobilisation or distraction at fracture site due to gravity. Tx: ORIF, bone grafting or intramedullary fibular graft. THen immobilise with shoulder spica or U slab.
Delayed union
Joint stiffness
Refracture
Q. What is Holstein Lewis Syndrome
Fractures of the distal third of the humerus with radial nerve paralysis
Radial nerve paralysis may be due to:
1) Nerve getting trapped at the fracture site
- Immediately following the fracture
-the nerve getting trapped during reduction of the fracture
2) Nerve getting trapped in the callus during healing of the fractures
Tx: Immediate ORIF
Radial Nerve Injury
Generally a neurapraxia only.
It may be sustained at the time of fracture, during manipulation of the fracture or while the fracture is healing (nerve entrapment in the callus)
The radial nerve injury results in paralysis of the wrist, finger and thumb extensors (wrist drop), brachioradialis and supinator. There is a sensory cahnge in a small area on the radial side of the back of the hand.
Tx: Most recover spontaneously. In open fractures, exploration usually required
In neglected cases or when repair of a divided nerve is impractical, tendon transfers are needed.
Modified Jone's transfer: muscles of forearm supplied by median nerve and ulnar nerves are used for substituting wrist extension, finger extension and thumb abduction extension. THe following tendons are used:
- Pronator teres--- extensor carpi radialis brevis
- Flexor carpi ulnaris--- extensor digitorum
- palmaris longus -----extensor pollicis longus
Great info
ReplyDeleteComminuted Fracture – Everything You Need to Know
Only a few types of fractures are associated with hip injuries, which cause back pain.
ReplyDeleteComminuted Fracture